
Author: Dr. Gabriel Mercadal Orfila | Department of Hospital Pharmacy, Mateu Orfila Hospital (Menorca, IB-SALUT)
For decades, we have measured health mainly through what can be captured in a blood test or an image: blood pressure figures, blood levels, millimetres of inflammation. These data are essential, but they tell only part of the story. What the health care system has rarely recorded in a structured way is precisely what matters most to people living with a chronic disease: how they feel, what they can and cannot do in their daily lives, and how they are treated by the very system that is meant to care for them.
That information exists, but it has traditionally been scattered across consultations, in isolated phrases that rarely became comparable, analysable data useful for decision-making. Recovering it systematically is the starting point of what we now call value-based health care, and it is also the raison d’être of the NAVETA program.
What PROMs and PREMs are – and why they matter
PROMs, or Patient-Reported Outcome Measures, are validated questionnaires that capture health outcomes directly from the patient’s own voice: pain, fatigue, quality of life, mood, functional capacity, or the impact of disease on their routine. They are not interpreted by a professional on the basis of a test; they are answered by the person themselves. This makes them the most faithful measure of what a treatment is truly intended to change.
PREMs, or Patient-Reported Experience Measures, capture something different but complementary: the patient’s experience of the care received. Whether they felt listened to, whether the information was clear, whether coordination between professionals worked, whether the care pathway made their life easier or more complicated. While the PROM answers “Am I better?”, the PREM answers “How was I cared for?”. It is also important to distinguish experience from mere satisfaction: satisfaction measures whether the patient was pleased; experience describes what actually happened at each point of their care journey – inside and outside the hospital – and is therefore much more actionable for improving processes (figure 1).
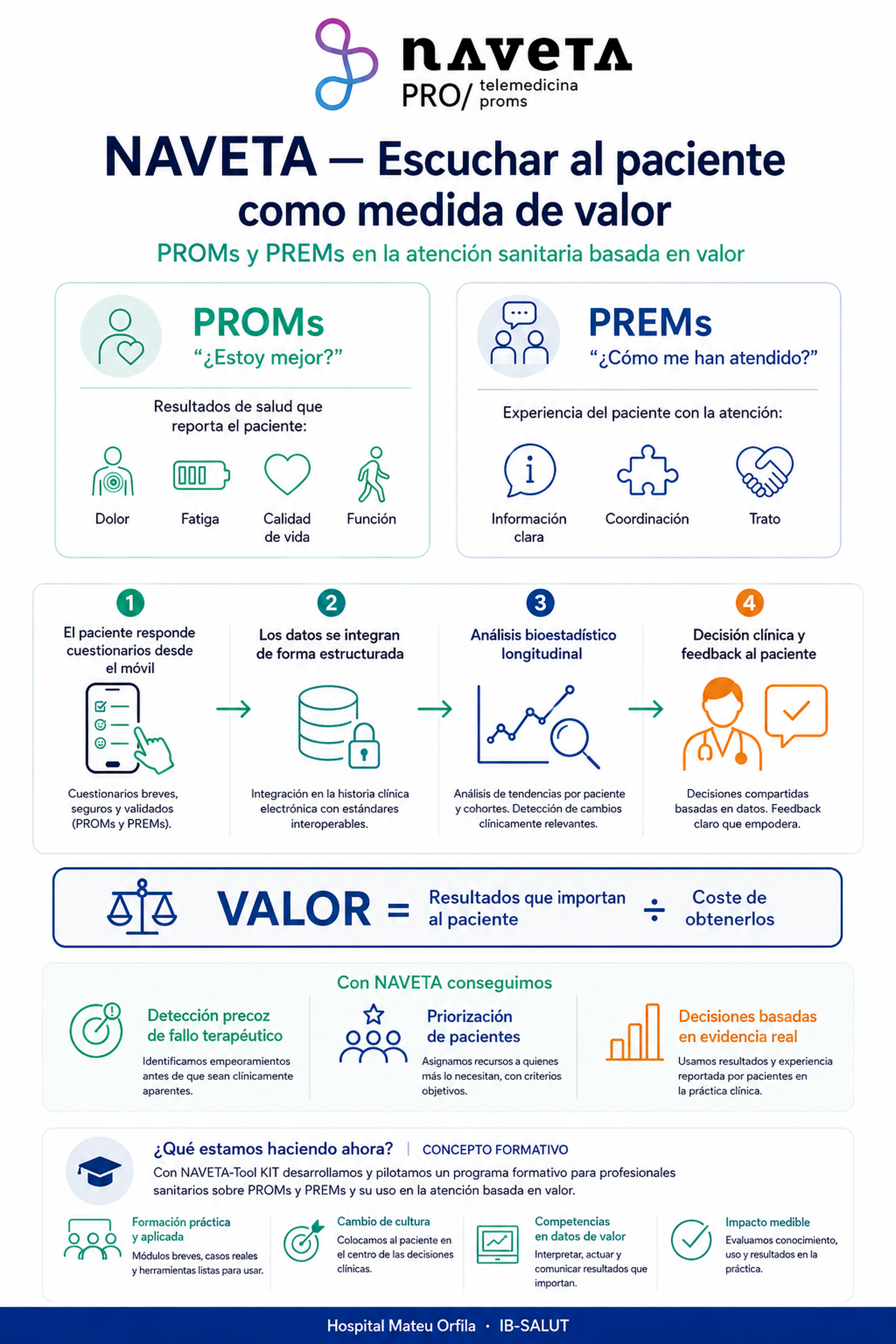
Figure 1. NAVETA: PROMs and PREMs in value-based health care.
Measuring both routinely changes the clinical conversation. It makes it possible to detect early on that a treatment is not delivering the expected benefit, even when analytical parameters appear correct; it helps prioritise patients who are doing worse without waiting for the next scheduled appointment; and it gives professionals an objective basis for deciding whether to maintain, adjust, or change a therapy. Taken together, they turn the patient’s perception into evidence (10,11,15).
NAVETA: placing the patient’s voice at the centre of follow-up
NAVETA is the outcomes and experience monitoring program for chronic patients that we have been developing in the Balearic Islands since 2021, with a multidisciplinary scientific committee comprising engineers, physicians, pharmacists, psychologists and other profiles. Its idea is simple to state and demanding to implement: to integrate the electronic collection of PROMs and PREMs – ePROMs and ePREMs – into routine patient follow-up, continuously and over time, rather than as a one-off snapshot (1,2).

How it works in practice
Patients complete validated questionnaires from their own device, at clinically relevant points in their treatment. These responses are incorporated into their follow-up in a structured way, analysed using rigorous biostatistical methodology, and returned in two directions: to the care team, which gains a longitudinal view of each person’s real evolution, and to the patient, who receives an understandable reading of their results.
The key is not only to ask questions, but to decide what is done with the answers. NAVETA is designed to cover a broad range of chronic diseases and the validated instruments specific to each one3,4,6,7. The program began in 2021 with psoriasis and now includes 26 PROM and PREM standard sets in areas such as rheumatology, dermatology and neurology – the most recent additions being vitiligo and obesity – so that follow-up is not limited to a single data point but instead describes a trajectory: when improvement appears, whether it is sustained over time, and whether it reaches a clinically relevant change for the patient, not merely a statistical variation.
Working with methodological rigour is an essential part of the project. It is not enough to accumulate questionnaires: it is necessary to ensure that each score comes from the correct instrument, to clean invalid values, to analyse evolution using models suited to real-world data – incomplete and uneven by nature – and to compare improvements against recognised thresholds of clinical relevance (5,8). Only in this way does the patient’s voice become robust evidence rather than noise.
This approach has gained momentum and external recognition. Since 2021, NAVETA and the projects derived from the initiative have received nine innovation awards in hospital pharmacy, telepharmacy and artificial intelligence: from the SEFH 2nd Innovation Forum Award in 2021 and the AMPHOS Pharmacy Award in 2022, to the 1st SEFH–CSL Vifor Award in 2025 for the ZAFIRO project, the Visionarium by Gilead Award in 2025 and the runner-up distinction at the 2026 Novartis–IESE Awards for excellence in health care management for NAVETA Dermatology, among others.
From data to decision-making: value-based care
Value-based health care proposes an idea that is as reasonable as it is transformative: measuring the success of the system not by the volume of activity it generates – tests, visits, medicines dispensed – but by the outcomes that truly matter to patients in relation to the resources used. In this logic, value is the quotient between the outcomes that are relevant to the person and the cost of achieving them (9).
This definition, formulated by Michael Porter, has evolved into a broader framework. The European Commission Expert Panel proposes a “quadruple value” model with four complementary pillars: personal value – care aligned with each patient’s goals; technical value – achieving the best possible outcomes with the available resources; allocative value – distributing those resources equitably across all patient groups; and societal value – the contribution of care to participation and social cohesion (16). PROMs and PREMs directly feed the first two pillars and provide the baseline information needed to evaluate the other two.
This equation is impossible to calculate if we only measure the traditional clinical numerator. Without PROMs, we do not know whether the patient is truly living better; without PREMs, we do not know whether the care process adds value or detracts from it. That is why both instruments are not an aesthetic add-on to the value model: they are its condition of possibility. They are the tool that allows “value” to stop being a slogan and become something that can be observed, compared and improved.
When this information is incorporated systematically, decisions change at every level. Clinicians adjust treatment based on data rather than impressions. Pharmacy departments identify which therapies provide real and sustained benefit and which do not justify their cost. And the system finally has real-world evidence to guide planning, funding and continuous improvement in care (12,13,14).
A specific example is the ZAFIRO project, a digital pharmacotherapeutic follow-up model in inflammatory bowel disease – awarded at the 2025 SEFH–CSL Vifor Awards – which applied this same PROM and PREM logic in 115 patients followed for 48 months. The results: a 22% increase in therapeutic adherence, a 45% increase in the detection of medication-related problems and a 27% reduction in face-to-face visits, with overall satisfaction of 9.2 out of 10 and 83% of patients reporting good quality of life. Measuring outcomes and experience does not merely describe care: it improves it.
In chronic patients, the value-based approach naturally converges with models of chronic care and integrated care: what is measured ceases to be an isolated episode and becomes the patient’s complete journey over time and across levels of care. Measuring outcomes and experience longitudinally is precisely what makes it possible to manage that journey, not merely document it.
A final reflection
Incorporating the patient’s perspective is not a kind concession or a health care marketing exercise: it is a methodological improvement that makes the system more precise, more efficient and fairer. It means recognising that no one knows the effect of a treatment better than the person receiving it, and that this information, when collected rigorously, is as valuable as any biomarker.
The challenge in the coming years will not be technological – the tools to collect ePROMs and ePREMs already exist – but cultural and organisational: turning listening into a structured habit of the system and, above all, into decisions that change patients’ lives. Programs such as NAVETA aim to contribute to this change from the ground up: one hospital, a group of patients and the conviction that measuring what matters is the first step towards improving it.
References
NAVETA Program – publications by the team
1. Mercadal-Orfila G, et al. Implementing Systematic Patient-Reported Measures for Chronic Conditions Through the Naveta Value-Based Telemedicine Initiative: Observational Retrospective Multicenter Study. JMIR Mhealth Uhealth. 2024. doi:10.2196/56196
2. Mercadal-Orfila G, et al. Person-Centered Coordinated Care Experience of People With Long-Term Conditions in the Balearic Islands Measured by the P3CEQ. Health Serv Insights. 2024. doi:10.1177/11786329241258856
3. Mercadal-Orfila G, et al. TELEPROM Psoriasis: Enhancing patient-centered care and health-related quality of life (HRQoL) in moderate-to-severe plaque psoriasis. Front Med. 2024. doi:10.3389/fmed.2024.1465725
4. Mercadal-Orfila G, et al. Patient-reported outcome measures for assessing atopic dermatitis in clinical practice. Farm Hosp. 2024. doi:10.1016/j.farma.2024.08.004
5. Mercadal-Orfila G, et al. Developing a Prototype Machine Learning Model to Predict Quality of Life Measures in People Living With HIV. Integr Pharm Res Pract. 2025. doi:10.2147/IPRP.S492422
6. Mercadal-Orfila G, et al. The NAVETA obesity consensus tool: a multidimensional framework for clinical and patient-reported outcome assessment. Front Endocrinol. 2026. doi:10.3389/fendo.2025.1731194
7. Mercadal-Orfila G, et al. Telepharmacy follow-up using ePROMs in moderate-to-severe psoriasis (TELEPROMpsoriasis). Farm Hosp. 2026. doi:10.1016/j.farma.2026.01.006
8. Mercadal-Orfila G, et al. Digital Monitoring of Pre-Exposure Prophylaxis Users Through ePROMs and ePREMs: Multicenter Prospective Study on Feasibility, Safety, and Predictive Modeling of Digital Engagement. J Med Internet Res. 2026. doi:10.2196/87592
Value-based care, PROMs and PREMs
9. Porter ME. What is value in health care? N Engl J Med. 2010;363(26):2477-2481. doi:10.1056/NEJMp1011024
10. Bull C, Teede H, Watson D, Callander EJ. Selecting and Implementing Patient-Reported Outcome and Experience Measures to Assess Health System Performance. JAMA Health Forum. 2022;3(4):e220326. doi:10.1001/jamahealthforum.2022.0326
11. Howell D, Molloy S, Wilkinson K, et al. Patient-reported outcomes in routine cancer clinical practice: a scoping review of use, impact on health outcomes, and implementation factors. Ann Oncol. 2015;26(9):1846-1858. doi:10.1093/annonc/mdv181
12. Varela-Rodríguez C, García-Casanovas A, Baselga-Penalva B, Ruiz-López PM. Value-Based Healthcare Project Implementation in a Hierarchical Tertiary Hospital: Lessons Learned. Front Public Health. 2022;9:755166. doi:10.3389/fpubh.2021.755166
13. Meregaglia M, Malandrini F, Angelini S, Ciani O. The Assessment of Patient-Reported Outcomes for the Authorisation of Medicines in Europe: A Review of European Public Assessment Reports from 2017 to 2022. Appl Health Econ Health Policy. 2023;21(6):925-935. doi:10.1007/s40258-023-00827-3
14. Hjollund NHI, Larsen LP, de Thurah AL, et al. Patient-reported outcome (PRO) measurements in chronic and malignant diseases: ten years’ experience with PRO-algorithm-based patient-clinician interaction (telePRO) in AmbuFlex. Qual Life Res. 2023;32(4):1053-1067. doi:10.1007/s11136-022-03322-9
15. Kotronoulas G, Kearney N, Maguire R, et al. What is the value of the routine use of patient-reported outcome measures toward improvement of patient outcomes, processes of care, and health service outcomes in cancer care? A systematic review of controlled trials. J Clin Oncol. 2014;32(14):1480-1501. doi:10.1200/JCO.2013.53.5948
16. Expert Panel on effective ways of investing in Health (EXPH). Opinion on defining value in “value-based healthcare”. Luxembourg: Publications Office of the European Union; 2019. doi:10.2875/35471